
The Tipping Point: COVID-19 Positions to End the Decades-long Battle for Telehealth Reimbursement

Explore how COVID‑19 accelerated telehealth reimbursement reform, overcoming longstanding barriers and paving the way for widespread virtual care adoption.
You don’t necessarily have to be in the healthcare industry to see that COVID-19 has changed the way we approach the delivery of healthcare services. From sending hospitals into and beyond surge capacity to canceling elective surgeries and disrupting supply chains, almost every facet of the industry has been affected, the results of which will have a ripple effect for years.
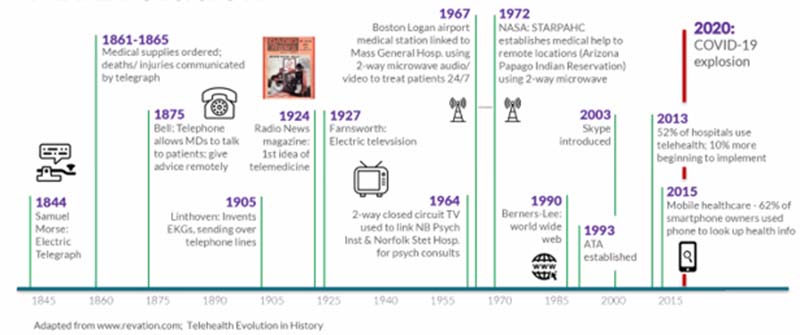
With disruption comes positive change, and one area seeing momentum is within the adoption of telehealth. For years, healthcare providers have attempted to improve patient access to care, as well as the overall cost of care, through telehealth adoption. Despite good intentions, payers have not supported telehealth as they did not see virtual visits as a proper supplement for, or even complement to, in-person care. Many providers have avoided the upfront capital cost of implementing broad telehealth systems for this reason.
In 2019, a large Midwest academic medical center (AMC) anticipated that 0.52%-6.68% of patients would utilize a telehealth video platform for live video consults, with the assumption that a 6.68% adoption rate would be aggressive. That changed in the spring of 2020.
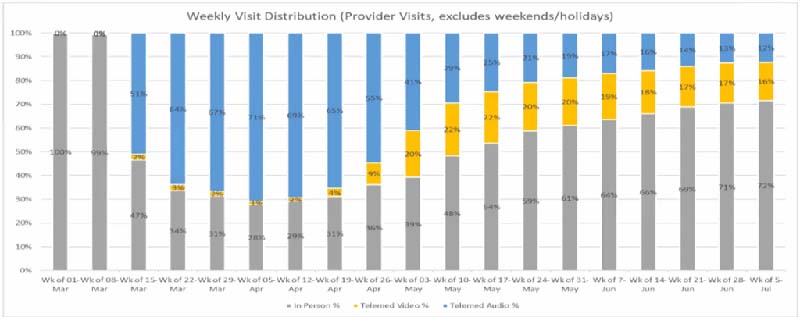
Under the CARES Act and a number of additional waivers (1,135 to be exact), CMS allowed payment flexibility during the pandemic, granting payment parity between telehealth and in-person clinical care for Medicare patients. The results were immediately apparent. The same AMC that anticipated an aggressive telehealth adoption rate of 6.68% saw an overnight jump in the use of telehealth – at first audio-based, then video-based. In the first week of April 2020, 72% of ambulatory patient encounters were done remotely via telehealth (primarily audio-based). By the first week of July 2020, 28% of patient encounters remained virtual and 16% of all patient encounters were video-based telehealth visits.
Telehealth use has fallen since the first waves of the pandemic; however, it is still drastically higher than anticipated even just eight months ago. Over 20% of patient encounters remain virtual, a signal providers and payers can’t ignore. Although we aren’t likely to fully adopt telehealth as a substitute for in-person care, we’re also unlikely to return to pre-pandemic levels. Providers, payers, and politicians are making the push for sustainable telehealth adoption and reimbursements. A U.S. House bill introduced in September 2020 (HR 8308) has proposed mandated payer coverage for telehealth services. Some states and payers have already moved to make the change permanent.
Telehealth is not a direct substitute for in-person care. However, it provides another convenient platform to access care and reduce the barrier to entry for many patients. Moving forward we must ensure that we leverage telehealth in productive ways to improve access to care, outcomes, and overall cost for all patients, especially for the most vulnerable. In doing so we can confront the unaffordability and inequity within primary and specialty care.
https://www.cdc.gov/coronavirus/2019-ncov/hcp/telehealth.html#edn10
https://www.ama-assn.org/practice-management/medicare/cms-payment-policies-regulatory-flexibilities-during-covid-19
Related News & Insights

The Fizz Factor: Learn Why CO2 Is Critical in Beverage Processing
Discover the science behind carbonated beverages and how Haskell SME Dwight Garrels helps clients optimize critical components of manufacturing.
60 Years of Bold Architectural Integration and Innovation
Explore how Haskell’s architects deliver integrated solutions across industries. Learn how purposeful design can elevate your next built environment.

Manufacturing Consultants Solve Process and Operational Challenges
Discover how manufacturing consultants solve real-world production challenges with smart, cost-effective strategies that drive measurable results.

Flip Rooms Maximize Physician Time and Enhance Hospital Revenue
Learn how a well-executed flip room strategy helps hospitals optimize surgery schedules, support physicians and improve patient experience.



