
Flip Rooms Maximize Physician Time and Enhance Hospital Revenue

Learn how a well-executed flip room strategy helps hospitals optimize surgery schedules, support physicians and improve patient experience.
The practice whereby a physician operates on patients in 2 overlapping rooms is called a flip room. The physician must be present during clearly identified critical portions of the procedure, typically the middle. Operating a flip room makes the physician more efficient by minimizing the time spent waiting for a case to turn over.
A physician can complete two days of cases in one day by moving between rooms. The time freed up allows the physician to perform more specialized procedures and training of fellows and residents (Wood, 2018). In addition, physicians can reclaim office time when they can see new/existing patients and bring in additional cases. The benefits of offering flip rooms to physicians improve recruitment and retention of in-demand physicians and service lines. Ultimately, it is about the patient experience, and operating an efficient flip room program can lead to completing cases on time and earlier in the day (Stocum, 2022).

The downfalls of flip rooms are reduced prime-time utilization, increased resource constraints and patient skepticism. With a staggered start, a hospital will see a reduction in prime-time utilization by upwards of 10% or more. This decrease reduces the hospital’s profitability because of the increase in non-revenue-generating minutes in the OR. An efficient flip room requires two teams, each comprising nurses, techs and adequate anesthesia coverage, additional equipment and trays, two ORs, and a physician. A patient must have full disclosure that a physician may be absent during parts of their procedures and have the right to refusal (Wood, 2018).
A flip room is a privilege for experienced surgeons who adhere to the policy and comply with metrics. Here are some key policies for consideration:
- Volume
- Physicians’ ability to average 6-7 cases per 8-hour block
- Case Length
- Short to medium case length
- Predictable case length with low variability
- Surgery time to case setup time as close to a 1:1 ratio
- Scheduling
- Schedule most difficult cases at end of the day
- Identify critical parts of the case that the attending must be in the room
- Scheduling like cases
- Patients
- Medically stable with a routine surgical procedure
- Resources
- Physician Assistants to assist in closing
- Capacity of additional tables, equipment, and teams to prep/clean room
- Metrics
- Establish a committee for monitoring and compliance
- Utilization of both rooms meets the policy of at least 70%
- Maintain first-case on-time starts of at least 90%
We looked at a medium-sized city regional hospital’s data for the yearlong period from July 1, 2022, to June 30, 2023, to identify the effect of prime-time utilization in operating flip rooms. We focused on the Orthopedics service line and performed an analysis of the period from 7:30 a.m. to 3:30 p.m. Monday through Friday. Prime-time utilization is the number of revenue-generating minutes divided by the total number of minutes available during normal business hours. Normal business hours are when the department is staffed and available to perform surgeries. Cases performed outside of normal business hours increase surgery costs because of overtime and inefficiencies (Tout & Ayres, 2022). What is the impact on prime-time utilization, and what factors contribute to this number?
For this hospital, we saw a prime-time utilization where there was at least one physician utilizing a flip room of 71.0% for Room 1 and 61.9% for Room 2. Room 1 is defined as the first scheduled case of the day for the physician and Room 2 is the next scheduled case in a different room.
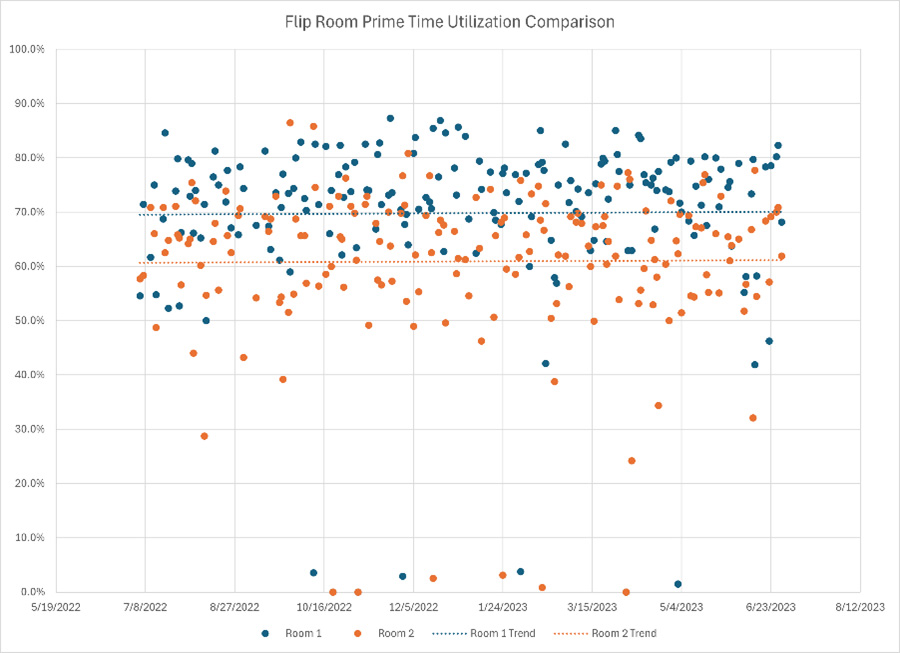
Overall, the delta in prime-time utilization between the two rooms was, on average, 9.1%. Over the course of a year, that equates to 10,200 fewer revenue-generating minutes. With an average case duration of 120 minutes, that equates to 85 cases per year. With an average estimated payment/claim for total knee and hip of $13,000 to $14,000, that is $1.1 million to $1.2 million in lost revenue.
What explains the lower utilization numbers in the second room? While first-case on-time start is important for both rooms, it is more important to get Room 2 started on time because of its staggered start. Look at Figure 1 and see all the empty time before the first case of the day. Starting a case late in Room 2 only exacerbates the reduction in prime-time utilization. Nearly 13.1%, or 1,340 minutes, contributed to the 9.1% in lost prime-time utilization. While the Room 1 first-case on-time start percentage is slightly lower than Room 2 at 67%, the delay associated with the late cases in Room 2 is much longer.
It’s more difficult to directly attribute room turnover time to prime-time utilization, but on average, Room 2 has a higher average by 6.2%. Room turnover time equals non-revenue generating minutes that are necessary to set up for the next case.
Flip rooms are a very effective way to recruit and retain in-demand physicians. They contribute to increased revenues for the hospital by improving time management and efficiencies for the physicians. Proper flip room scheduling is critical to optimizing use and maximizing revenue generation. Hospitals are wise to create a committee to develop, implement, monitor and enforce the most effective policy possible.
Stocum, Elizabeth (2022, November 17). Challenges and Best Practices with Strategizing Flip Rooms. Retrieved from OR Manager: https://www.ormanager.com/challenges-and-best-practices-with-strategizing-flip-rooms/
Trout, Austin & Ayres, Catherine (2022, April 29). Why Focus on Operating Room Prime Time Utilization: A Metric for Better Use of OR Time. Retrieved from LeanTaaS: https://leantaas.com/blog/why-focus-on-operating-room-prime-time-utilization-a-metric-for-better-use-of-or-time/
Tse, Debra (2023, November 14). OR “Flip Rooms” are Nothing to Flip Out About. Retrieved from LeanTaaS: https://leantaas.com/blog/or-flip-rooms-are-nothing-to-flip-out-about/
Wood, Elizabeth (2018, December 13). Policy Compliance Essential for Overlapping Surgery Safety. Retrieved from OR Manager: https://www.ormanager.com/policy-compliance-essential-overlapping-surgery-safety/
 About the author: Nick Brown is a Senior Consultant at Haskell. With over 10 years of experience in data analytics, process improvement and programming. He specializes in developing and delivering innovative solutions using Power BI and simulation modeling to help healthcare organizations achieve their strategic goals and optimize their resources. He has a bachelor’s in Business Administration from The Ohio State University, a Master’s of Science in Human Factors Engineering from Wright State University and multiple Lean Six Sigma certifications.
About the author: Nick Brown is a Senior Consultant at Haskell. With over 10 years of experience in data analytics, process improvement and programming. He specializes in developing and delivering innovative solutions using Power BI and simulation modeling to help healthcare organizations achieve their strategic goals and optimize their resources. He has a bachelor’s in Business Administration from The Ohio State University, a Master’s of Science in Human Factors Engineering from Wright State University and multiple Lean Six Sigma certifications.
Related News & Insights

The Fizz Factor: Learn Why CO2 Is Critical in Beverage Processing
Discover the science behind carbonated beverages and how Haskell SME Dwight Garrels helps clients optimize critical components of manufacturing.
60 Years of Bold Architectural Integration and Innovation
Explore how Haskell’s architects deliver integrated solutions across industries. Learn how purposeful design can elevate your next built environment.

Manufacturing Consultants Solve Process and Operational Challenges
Discover how manufacturing consultants solve real-world production challenges with smart, cost-effective strategies that drive measurable results.

System Analytics Leader Recognized with Pair of INFORMS Honors
Join us in celebrating Shannon Browning's new Senior Member status in the organization and learn how she earned its Volunteer Service Award.



