
Integrating Behavioral Health into Your Primary Care Clinic

Discover why integrating behavioral health services into primary care clinics improves access and how to design spaces and workflows to support it.
As behavioral health disorders become more prevalent and rise as a national priority, transforming our thinking on when and how we provide care for behavioral health patients is unavoidable. A recent blog post Community Matters for Behavioral Health Patients references a need for 123,300 psychiatric beds to fill the current shortage, meaning that emergency departments are often the first line of care for these patients. However, the ED not only is the most expensive site of care but also is not conducive to care for most behavioral health patients.
The shift in where and how behavioral health is treated is progressing, and primary care is at the forefront of multiple avenues for proactively identifying and treating behavioral health patients. But what is the best way for primary care clinics to integrate these services into their practices?
In our experience, there are three primary care models that you can use to integrate behavioral health into the clinic setting.
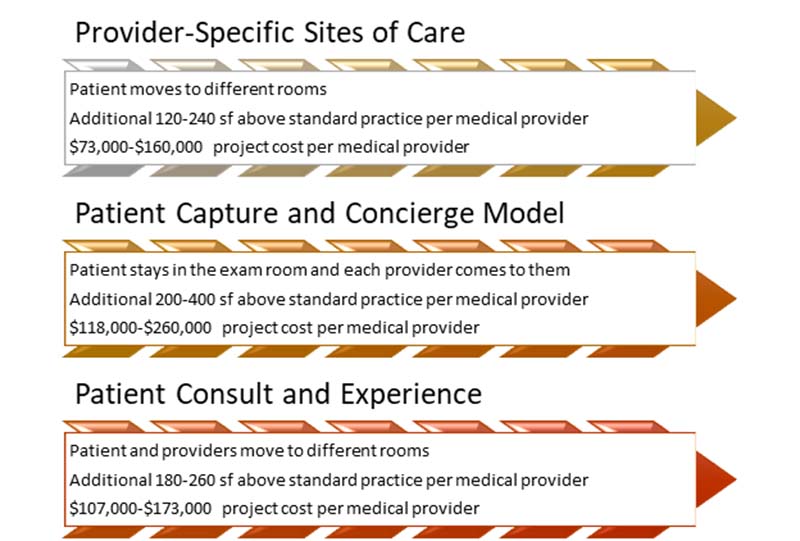
Provider-Specific Sites of Care
This model of care is formulated around providers each having their own location to provide care. In other words, the patient would see the primary care provider in an exam room. If the PCP determines the patient needs to speak with a behavioral healthcare provider, the patient would then move to the behavioral health provider’s office to free up the exam room so the PCP can maintain productivity and minimize scheduling issues. The provider-specific sites of care model:
- Minimizes building additional expensive exam rooms
- Focuses on providing care based on the setting most appropriate for the provider
- Creates the opportunity for patients to leave through “bus stops”
- May require a sub-wait component, with moderate to limited flexibility for scheduling
Patient Capture and Concierge Model
This model of care hinges on the idea that the patient doesn’t move through the primary care clinic. Instead, the various providers come to the exam room to see the patient while having their own offices or workspaces. The patient capture and concierge model:
- Requires more exam rooms be built per provider, significantly raising the cost
- Focuses on capturing the patient and minimizing their movement to other spaces (“bus stops”)
- Reduces the opportunity for patients to leave
Does not utilize sub-wait but has a greater potential to affect provider throughput, scheduling, and other patients - Loses opportunity to create a good environment for behavioral health discussions given the design requirements of exam rooms but meets the overall need
- Great for concierge models for patient satisfaction as well as for clinics serving indigent populations where there are inherently compliance, access, and resource challenges
Patient Consult and Experience
A bit of a hybrid between the first two models, the patient moves between the exam room and a consult room, but the consult room is smaller and more conducive to care while the providers also have their own offices or work space. The patient consult and experience model:
- Minimizes building additional expensive exam rooms
- Focuses on providing an appropriate environment of care for the patient and the experience
- Creates an opportunity for patients to leave through “bus stops”
- May require a sub-wait component but also provides the greatest amount of flexibility with scheduling
- Creates an opportunity to create healing consult rooms that are comfortable and use calming and soothing design attributes
Care Isn’t Limited to the Clinic
The patient encounter doesn’t start at the in-person visit but rather with a pre-visit screening questionnaire. This questionnaire can help providers identify whether a behavioral health consult is needed, which can help in scheduling and minimize excess square footage that is programmed out of uncertainty. Surveys and pre-visit screenings are a great way for rural or small clinics as well as large urban clinics, which may not be able to employ behavioral health providers, to schedule behavioral health tele-consults with patients during their visit. Each model of care can be complemented with follow-up communications via phone calls, emails, texts, or surveys to help confirm patients are complying with treatment and connecting with additional resources.
Many populations in which behavioral health disorders, ranging from substance abuse to personality issues, are prevalent are more likely to have less access to other resources:
- Financial counseling
- Transportation
- Access to behavioral health resources
- Nutrition and exercise
- Shelter
- Medicine and pain management
By addressing some of the issues that often go hand-in-hand with behavioral disorders, providers can better manage the wellness of their community. This is where providers can help patients navigate and connect with other programs and community groups with great resources.
In the primary care setting, finding the best way to help the community takes some planning and a vision. Finding a way to integrate behavioral health into your primary care clinic can lessen the burden on emergency services and offer intervention for patients before their situation becomes critical.
Related News & Insights

The Fizz Factor: Learn Why CO2 Is Critical in Beverage Processing
Discover the science behind carbonated beverages and how Haskell SME Dwight Garrels helps clients optimize critical components of manufacturing.
60 Years of Bold Architectural Integration and Innovation
Explore how Haskell’s architects deliver integrated solutions across industries. Learn how purposeful design can elevate your next built environment.

Manufacturing Consultants Solve Process and Operational Challenges
Discover how manufacturing consultants solve real-world production challenges with smart, cost-effective strategies that drive measurable results.

Flip Rooms Maximize Physician Time and Enhance Hospital Revenue
Learn how a well-executed flip room strategy helps hospitals optimize surgery schedules, support physicians and improve patient experience.



